Adolescent Mental Health Care Is Its Own System
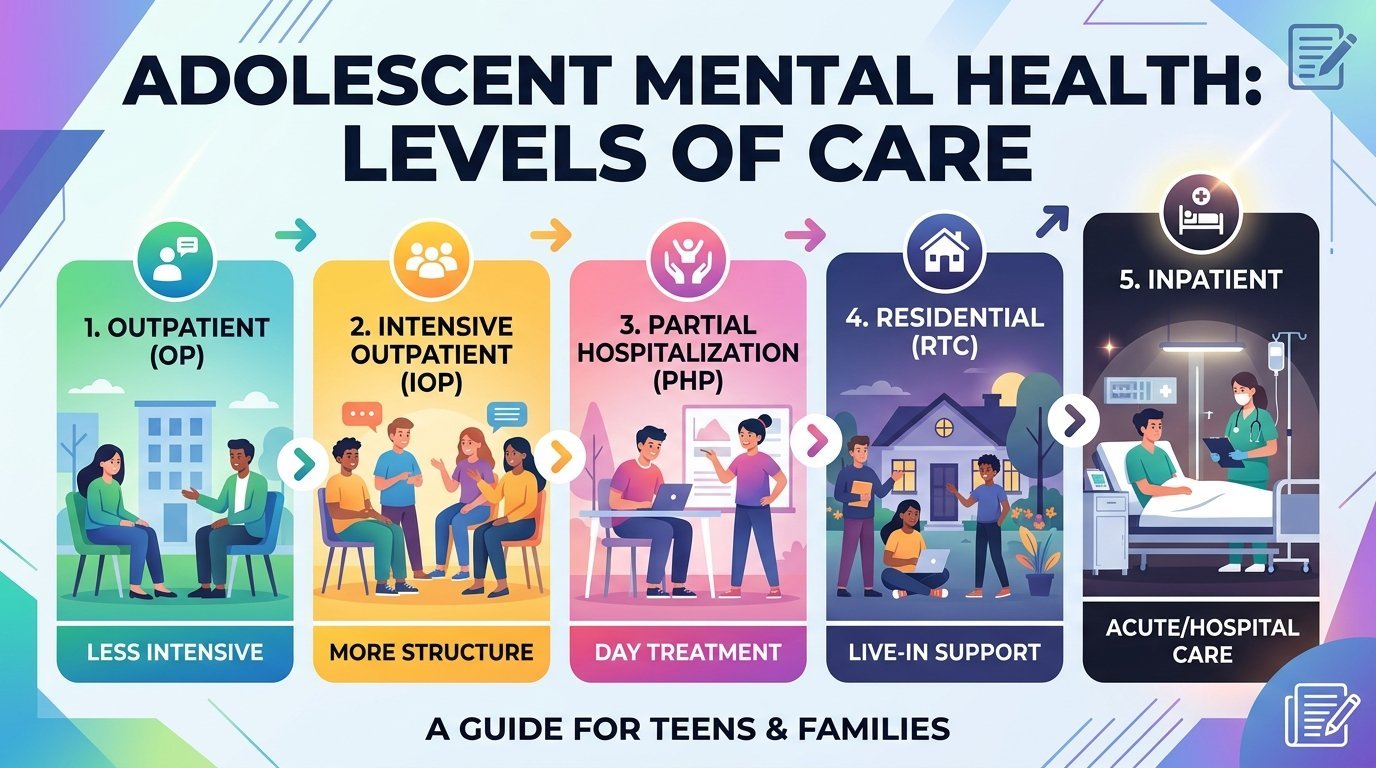
The continuum of mental health care for adolescents looks superficially similar to the adult continuum, with outpatient therapy, intensive outpatient, partial hospitalisation, residential, and inpatient levels. The actual experience inside each level is dramatically different. Adolescent programs incorporate school components, family work, developmental considerations, and identity-formation issues that adult programs do not address. Parents who try to navigate adolescent treatment with adult-system intuitions often miss important distinctions.
This guide describes adolescent levels of care specifically, including what each level looks like for teens, when each is the right choice, how schools fit in, and how insurance and family decisions interact. The audience is parents and caregivers approaching this system for the first time, often during a moment of significant family stress.
Adolescent Outpatient Therapy
Standard outpatient therapy for adolescents typically involves weekly individual sessions with a therapist who specialises in working with teens, often supplemented by occasional family sessions. The therapist’s job is more complex than in adult therapy because the patient is still developmentally forming, the parents are still legally responsible, and school is still a daily life context. The good adolescent therapist holds all three frames at once.
Confidentiality is structured differently for minors. The therapist maintains a working relationship with the adolescent that includes some level of confidentiality, while keeping parents informed about general treatment progress and any safety concerns. The structure is described to parents at the start of treatment. Parents who try to extract detailed session content typically undermine the therapy. Parents who respect the structure while staying engaged in family sessions and treatment planning typically support strong outcomes.
Most adolescent mental health providers near me will accept commercial insurance, Medicaid, and CHIP coverage. Networks behind UnitedHealthcare therapists, Aetna therapists, Cigna therapists, and Blue Cross Blue Shield variants all operate adolescent specialty panels. The supply of adolescent-trained clinicians is thinner than for adults in most regions, particularly for younger adolescents and those with complex presentations.
Adolescent Intensive Outpatient Programs
Adolescent IOPs run nine to twelve hours per week, often three afternoons per week after school, for six to twelve weeks. The cohort model is essential. Teens benefit enormously from working with peers facing similar challenges, in a structured group environment that combines therapy, skills training, and educational components. The cohort itself is part of the treatment, normalising experiences that the adolescent had felt alone with.
Adolescent IOPs typically include parent components built into the schedule, often a weekly parent group or family session. The integration matters. Adolescent symptoms develop in family contexts, and family work is among the strongest predictors of long-term outcome. Programs that minimise the parent component tend to produce shorter durability of gains. Programs that engage parents seriously tend to produce more lasting change.
Common indications for adolescent IOP include moderate-to-severe depression that is not improving with weekly therapy, anxiety with significant school refusal or social impairment, substance use that has not responded to outpatient treatment, eating disorders in early-stage presentation, post-discharge stabilisation from inpatient psychiatric admission, and self-harm without immediate safety concerns. The level is increasingly used as a first step up from outpatient when symptoms have progressed beyond what weekly therapy can manage.
Adolescent Partial Hospitalisation Programs
Adolescent PHPs run six hours per day, five days per week, typically for two to four weeks. Most include a school component, with academic work supervised by the program staff so the adolescent does not fall further behind. The integration of treatment and education is one of the most useful features of adolescent PHP, because school disruption is often a major contributor to the adolescent’s functional impairment.
Adolescent PHP is most often used after an inpatient discharge, or as a step up when adolescent IOP has not produced sufficient stabilisation. The increased intensity allows for daily clinical contact, more comprehensive family work, and tighter medication management when needed. Length of stay is usually shorter than for adults, since adolescents generally stabilise more quickly when given structured mental health care and a removed-from-home environment during the day.
Adolescent Residential Treatment
Adolescent residential treatment is one of the more controversial parts of the system. The treatment model removes the adolescent from home and from school for an extended period, typically thirty to ninety days, though some programs offer significantly longer stays. The argument for residential treatment is that some adolescents cannot stabilise in their home environment, often because the home environment itself is part of the problem, and need a complete interruption to engage with treatment.
Indications for adolescent residential treatment include severe substance use disorders, severe and treatment-resistant eating disorders, complex post-traumatic stress disorder with home-based triggers, severe and persistent self-harm or suicidality not responding to outpatient or intensive levels, and adolescents whose families cannot provide the safety container needed for outpatient treatment to work. The level is also sometimes used for adolescents whose academic and behavioural deterioration has been severe enough that an extended therapeutic milieu is genuinely needed.
The controversy comes from the wide variation in program quality. Reputable adolescent residential programs operated by major academic medical centres or established non-profits provide evidence-based mental health care in a clinically governed setting. Less reputable programs, particularly some operating in the so-called troubled teen industry, have produced documented harms over the past several decades. Parents considering adolescent residential treatment should research specific programs carefully, ask for accreditation status, ask about staff training and supervision, ask about specific treatment modalities, and consult with the adolescent’s existing clinical team before committing.
Inpatient Psychiatric Hospitalisation for Adolescents
Adolescent inpatient admissions are typically short, three to seven days, and focus on stabilisation rather than long-term treatment. Reasons for admission include immediate suicidal danger, severe psychotic symptoms, severe agitation or aggression that cannot be managed safely at home, or severe substance withdrawal. The unit is locked, staff supervision is twenty-four hours, and family involvement is structured around brief visiting hours and family sessions.
The transition from inpatient to a step-down level is the most important phase of adolescent inpatient treatment. Most adolescents discharge to PHP or IOP for several weeks before returning to standard outpatient. The discharge planning ideally begins within twenty-four hours of admission and includes the family, the existing outpatient clinician, the school, and any community supports. Insurance preauthorisation for the step-down level is typically handled by the inpatient social worker.
School Coordination Across Levels
School is part of the treatment ecosystem at every level of adolescent mental health care. Outpatient therapy may include occasional consultation with the school counsellor or teacher. Intensive outpatient often involves coordinating absences for program attendance. Partial hospitalisation includes school components within the program schedule. Residential treatment requires educational continuity planning during the stay and reintegration planning at discharge.
Parents should expect to coordinate explicitly between the treatment team and the school. Many adolescents qualify for a Section 504 plan or an Individualised Education Program based on mental health conditions affecting their education. The plans formalise accommodations that support learning during and after treatment. The school’s responsibility to maintain access to education during a hospitalisation or residential stay is often greater than parents realise.
A Final Word for Parents
Navigating adolescent levels of care is hard. The decisions are weighty, the system is opaque, and the parent’s own emotional response to a child in crisis often complicates clinical thinking. The most helpful posture is to lean on the existing clinical team, ask explicit questions about the level of care being recommended and why, and trust the process while staying engaged. Adolescents whose parents engage seriously with treatment, including their own family role in it, generally do better than adolescents whose parents stay distant.
The recovery arc for adolescents is often quicker than for adults at comparable acuity, because the developmental window favours change. The investment of family attention, time, and resources in a difficult adolescent moment frequently produces durable change that supports the rest of the young person’s life. The work is real. So is the return.
This article is for educational purposes and does not replace personalised guidance from licensed clinicians. If your adolescent is in crisis, call or text 988 in the United States, or go directly to your nearest emergency department.